At the Veterinary Dental Center of Atlanta, we understand the importance of providing the best possible care for cats suffering from tooth resorption. Unfortunately, this condition often goes undiagnosed, as it can be difficult to detect without proper diagnostic tools.
Tooth resorption is a painful condition that occurs when the body’s cells begin to break down and digest the tooth from the inside out. Left untreated, it can cause severe oral pain and lead to tooth loss.
The key to proper diagnosis and treatment of tooth resorption is through full mouth veterinary dental radiographs. Our highly trained and experienced veterinary dental team use state-of-the-art technology and equipment to ensure that your cat receives the best possible care.
At the Veterinary Dental Center of Atlanta, we are committed to providing the best possible care for cats suffering from tooth resorption. Trust our team of experts for accurate diagnosis and effective treatment for your feline friend.
Prevalence
The combined gross and radiographic occurrence of tooth resorption in random populations of clinically healthy cats ranges from 29 to 38 percent.1-4 The number presenting to veterinary facilities primarily for dental disease is as much as twice as high.5,6
Many gross lesions are small and not readily detectable by awake oral examination alone. Magnification, immobilization and lighting generally provide a thorough gross evaluation but will not uncover tooth resorption below the level of the marginal bone. Therefore, dental radiography is paramount in establishing an adequate diagnosis.

Photo 1:
A triangular-shaped defect in the tooth at the gingival margin (arrow) is evident. This generally occurs in Type 1 and longer-standing Type 2 tooth resorption in cats.
Classification
One of the most useful clinical classifications of tooth resorption in cats to date is based on the gross and radiographic description of the lesions by type. Treatment is solely dependent on this type of classification, so, again, dental radiography is essential in making a final determination.
Grossly, Type 1 tooth resorption in cats is characterized by gingivitis and periodontitis generally initiated at the junction between the cementum and the enamel. The origin is thought to be inflammatory. Cavitation defects are seen in the crown, with inflamed gingival tissue often covering the defect (Photo 1). Radiographically, these teeth have variations in density in the crown or root. A distinct periodontal ligament space is generally appreciated (Photo 2). Type 1 and Type 2 tooth resorption may be observed concurrently in individual roots of a single tooth (Photo 3). Therefore, diagnostic evaluation of each root is important to determine how each should be approached therapeutically.
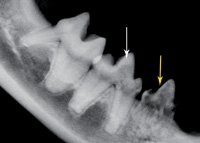
Photo 2:
The right mandibular fourth premolar, tooth 408 (white arrow), has a subtle crown lucency but an intact periodontal ligament space surrounding the roots consistent with Type 1 tooth resorption. The third premolar, tooth 407 (yellow arrow), has more pronounced crown lucency and no discernable periodontal ligament space surrounding the roots, which is typical of Type 2 tooth resorption.
Type 2 (Photos 2 and 3) tooth resorption is generally thought to start at the apical half of the root. Crown involvement is generally not noted until late in the resorption process. The hallmark of Type 2 tooth resorption in cats is the lack of radiographic evidence of a periodontal ligament space surrounding the root.
Treatment
Roots classified as undergoing Type 1 tooth resorption in cats require the removal of the entire tooth root and crown by using traditional extraction techniques (Photo 4). Tooth roots for which no periodontal ligament space is readily detected and where no periodontal bone destruction or periapical lucencies exist may be treated by crown amputation and intentional root retention. In these cases, a conservative periodontal flap exposes the marginal extent of the tooth (Photo 5), and a round carbide or diamond bur on a water-cooled, high-speed handpiece is used to remove the crown and contour the bone (Photo 6) before closure with 5-0 absorbable suture (Photo 7).
Exceptions exist for these generalizations regarding Type 2 lesions. Some roots may require partial extractions (more significant root remnant removal) if the periodontal ligament space is minimally detectable radiographically or abnormal tissue exists grossly upon exposure (consider biopsy in this instance). This includes friable tooth remnants. If there’s a bleeding pulp, the entire root should be removed.

Photo 3:
The left mandibular third premolar, tooth 307 (arrow), demonstrates both types of tooth resorption. The mesial root has a periodontal ligament space consistent with Type 1 tooth resorption. The distal root has an indistinguishable periodontal ligament space and resembles Type 2 resorption.
Photo 4:
A postoperative radiograph of the patient from Photo 2. Treatment for tooth 408 is complete extraction (Type 1). Treatment for tooth 407 is crown amputation and intentional root retention (Type 2).

Photo 5:
An example of a conservative periodontal flap. The marginal extent of tooth 307 is exposed using a periosteal elevator, followed by crown amputation with intentional root retention for treatment of Type 2 tooth resorption.

Photo 6:
The radiographic appearance of tooth 307 (same patient as Photo 5) after the use of a round carbide or diamond bur on a water-cooled, high-speed handpiece to remove the crown and contour the bone before closure.
Research and Prevention
Although causes have not been determined for tooth resorption in cats in general, one study suggests that cats with tooth resorption have significantly higher serum concentrations of 25-hydroxyvitamin D than cats do without tooth resorption.7 These researchers also found that 41 percent of canned cat foods have in excess of 30 times the vitamin D requirements of cats.8 Feeding diets that meet but don’t exceed the 250 IU/kg dry weight equivalent may prove to be a key to preventing tooth resorption. It’s also generally thought that Type 1 resorption is of inflammatory origin, so good oral hygiene may be key to preventing this form of resorption.

Photo 7:
Closure of the periodontal flap created to remove tooth 307 (same patient as Photos 5 and 6) using a 5-0 monofilament suture material.
Conclusion
The importance of dental radiography cannot be overstated but neither can the physical observation of the tooth root upon exposure. Consequently, veterinary practices that don’t have dental radiography and adequate surgical magnification shouldn’t be treating tooth resorption in cats. Either obtaining the proper equipment and training or referring to a specialist are the only feasible options for evaluating and treating these patients. Congratulations if your practice is effectively evaluating and treating these important feline oral defects.
References
1. Lund EM, Bohacek LK, Dahlke JL, et al. Prevalence and risk factors for odontoclastic resorptive lesions in cats. J Am Vet Med Assoc 1998;212(3):392-395.
2. Ingham KE, Gorrel C, Blackburn J, et al. Prevalence of odontoclastic resorptive lesions in a population of clinically healthy cats. J Small Anim Pract 2001;42(9):439-443.
3. Pettersson A, Mannerfelt T. Prevalence of dental resorptive lesions in Swedish cats. J Vet Dent 2003;20(3):140-142.
4. Girard N, Servet E, Biourge V, et al. Feline tooth resorption in a colony of 109 cats. J Vet Dent 2008;25(3):166-174.
5. van Wessum R, Harvey CE, Hennet P. Feline dental resorptive lesions. Prevalence patterns. Vet Clin North Am Small Anim Pract 1992;22(6):1405-1416.
6. Lommer MJ, Verstraete FJ. Prevalence of odontoclastic resorption lesions and periapical radiographic lucencies in cats: 265 cases (1995-1998). J Am Vet Med Assoc 2000;217(12):1866-1869.
7. Reiter AM, Lyon KF, Nachreiner RF. Evaluation of calciotropic hormones in cats with odontoclastic resorptive lesions. Am J Vet Res 2005;66(8):1446-1452.
8. Gawor JP, Reiter AM, Jodkowska K, et al. Influence of diet on oral health in cats and dogs. J Nutr 2006;136(7 Suppl):2021S-2023S.